Trastuzumab Emtansine
Overview
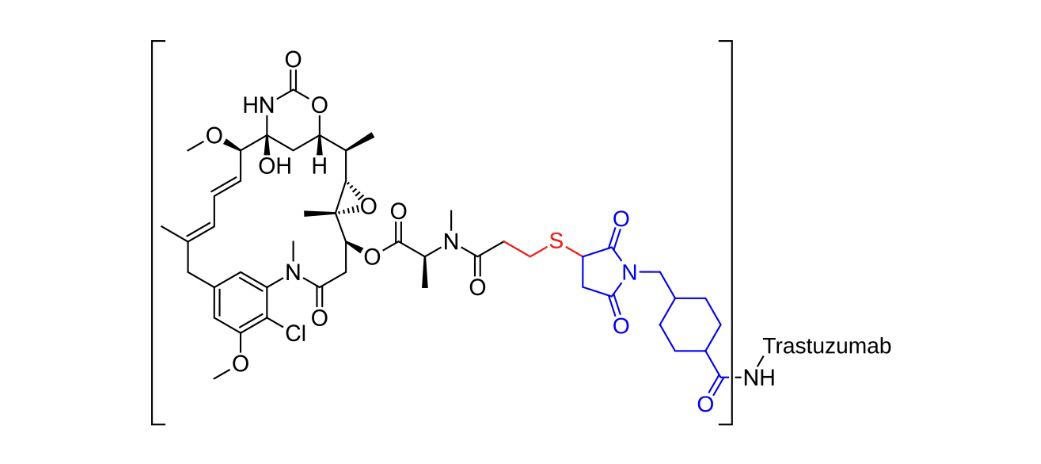
Trastuzumab emtansine (also known as ado-trastuzumab emtansine or T-DM1) is a targeted antibody–drug conjugate combining the HER2-directed monoclonal antibody trastuzumab with DM1, a potent cytotoxic agent. It specifically binds to HER2 on cancer cells, internalizes, and delivers DM1 directly where it disrupts microtubule function, leading to cell death. Available as an intravenous infusion, it is used in HER2-positive breast cancer patients who have received prior trastuzumab and a taxane, as well as for early-stage breast cancer with residual disease after neoadjuvant therapy. The drug has ushered in a new paradigm in oncology by delivering chemotherapy selectively to tumor cells, reducing systemic toxicity while improving outcomes.
Background and Date of Approval
Trastuzumab emtansine was first approved by the U.S. Food and Drug Administration in February 2013 for HER2-positive metastatic breast cancer following treatment with trastuzumab and a taxane, based on the pivotal EMILIA trial demonstrating significant survival benefit. It received European approval shortly thereafter and was later approved in the EU and other countries. In May 2019, FDA expanded approval for adjuvant use in early-stage HER2-positive breast cancer with residual invasive disease after neoadjuvant trastuzumab-based treatment, following the KATHERINE trial results showing a 50% reduction in risk of recurrence or death. These approvals have cemented its role across multiple stages of HER2-positive breast cancer treatment.
Uses
Trastuzumab emtansine is indicated for the treatment of adult patients with HER2-positive metastatic breast cancer who have previously been treated with trastuzumab and a taxane in either the adjuvant or metastatic setting. In early-stage disease, it is indicated as adjuvant therapy for patients with residual invasive disease following neoadjuvant chemotherapy including trastuzumab. It offers targeted, effective therapy for high-risk patients in both metastatic and early-stage disease where standard treatment leaves persistent cancer.
Administration
The recommended dose of trastuzumab emtansine is 3.6 mg/kg administered via intravenous infusion every three weeks. For early breast cancer, treatment continues for up to 14 cycles unless disease recurrence or unacceptable toxicity occurs. The infusion typically lasts about 30 to 90 minutes. Patients should be monitored for infusion reactions, and liver function tests—including transaminases and bilirubin—should be assessed before each dose. In the event of significant liver toxicity or cardiac function decline, dose interruption or adjustment may be necessary.
Side Effects
Patients commonly experience fatigue, nausea, elevated liver enzymes, musculoskeletal pain, hemorrhage, thrombocytopenia, headache, peripheral neuropathy, and arthralgia. Many of these effects are manageable and reversible with appropriate monitoring. The safety profile reflects the targeted nature of the drug and the early intervention strategies employed to mitigate side effects.
Warnings
Trastuzumab emtansine carries a risk of liver toxicity, cardiotoxicity through reduced left ventricular ejection fraction, and potential embryo-fetal harm, requiring effective contraception during and after treatment. It may cause serious or life-threatening effects such as severe hepatotoxicity and heart failure, necessitating pretreatment evaluation and on-treatment monitoring. The drug must be withheld in cases of severe toxicity and resumed cautiously.
Precautions
Patients must be evaluated for baseline liver and cardiac function before starting therapy. Concomitant use with liver-metabolized agents that increase AST, ALT, or bilirubin should be approached with caution. Given the risk of embryo-fetal toxicity, appropriate family planning advice should be provided. No significant pharmacokinetic drug-drug interactions have been noted outside of hepatic metabolism, but clinical vigilance is advised.
Expert Tips
Ensure liver enzymes and cardiac function are assessed before and during treatment. Educate patients to report symptoms such as jaundice, shortness of breath, or palpitations immediately. Use infusion-toxicity protocols and arrange supportive care accordingly. Coordinate closely with oncology and cardiology teams when managing patients with borderline heart function. For early-stage patients, counsel them on the importance of completing up to 14 cycles if tolerated.